
Have you ever hurt your ankle playing sport and are struggling to walk? Your walking is not improving, and it feels different to a normal ankle sprain? Maybe you have a fracture? Or is it a syndesmosis injury?
What is a Syndesmosis Injury?
A syndesmosis injury is typically known as a high-ankle sprain and is commonly seen in athletic populations, accounting for 11-17% of all ankle sprains (Brukner & Khan, 2017). It is an injury to the ligaments that stabilise the long bones of your lower leg (fibula and tibia) at the ankle joint. Its job is to keep these bones together at the ankle joint, helping to prevent them from splitting apart or separating while you walk, run and jump.
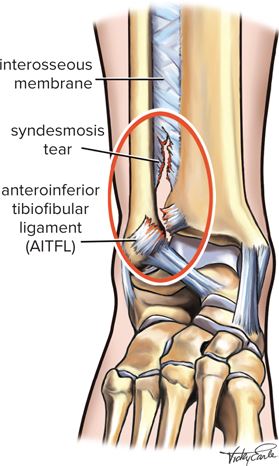
The syndesmosis can be categorised into different sections:
- The front of the syndesmosis consists of the anterior-inferior tibiofibular ligament (AITFL)
- The middle part is attached by the interosseous ligament (IOL)
- The back of the syndesmosis includes the posterior-inferior tibiofibular ligament (PITFL), and the transverse tibiofibular ligament (TTFL)
These structures work together with the other ankle ligaments to prevent widening of shin bones (fibula and tibia). This causes pain and instability, and if not diagnosed or treated correctly can cause long term issues in the ankle joint.
Ref: Brukner & Khan’s Clinical Sports Medicine
How does this injury occur?
This injury is often associated with a twisting injury to the ankle, particularly when the foot is rotated outwards and landed on heavily. It can also be caused when the foot is forced upwards (into dorsiflexion). These positions lead to a forceful widening of the joint, tearing the ligaments that hold the long shin bones together. Increased severity and force can tear the through majority of the ligaments and cause a fibula fracture (Maisonneuve Fracture) and lead to pronounced instability.
Who is at risk of a syndesmosis injury?
- Males are 3x times more likely to have a syndesmosis injury than females
- Sports involving boot immobilisation such as skiing and ice hockey
- Collision sports – e.g. include football, rugby, wrestling
- Higher level of athletic competition
- Previous history of ankle ligament tears
- Incomplete previous ankle rehab

What are the symptoms?
- Patients report pain in the ankle which is often felt higher up above the joint
- Poor ability to “push off” when walking and reduced ability to weight bear
- Audible pop or crack at time of injury
- Ankle swelling around the outside of the ankle, gradually increasing over the first two days (Hubbard et al, 2008)
- Bruising around the ankle is typically present
How is it diagnosed?
Physiotherapy, first and foremost, plays an important role in accurately assessing and diagnosing a syndesmosis injury. This is particularly important due to the poor outcomes associated with mismanaged/misdiagnosed syndesmosis injuries. Initially our physios will conduct a thorough examination and assessment. Information like the location of injury, mechanism of injury, type of sport or activity involved in, position of limb during the injury, and ability to bear weight after the injury will provide our physiotherapists with additional clues that help us make a proper diagnosis.
When suspicious of a syndesmosis injury, our physios will refer on for appropriate imaging which may include a weight bearing x-ray and/or MRI. On a weight bearing x-ray you can often see separation of the tibia and fibula but this depends on the severity of the injury. MRI gives further detail and clarity on the extent of the damage to the whole ankle joint.
Syndesmosis injuries can be classified into 3 Grades:
Grade I: Interosseous ligament & potential deltoid ligament injury, tenderness over AITFL. There is typically no separation on x-ray and a stable syndesmosis is present on clinical tests
Grade II: Complete AITFL & interosseous ligament tears present, but a normal x-ray may be present. On clinical testing an unstable syndesmosis may be present and confirmed via an MRI
Grade III: Complete injury to AITFL, PITFL, interosseous ligament and deltoid ligament avulsion, separation noted and unstable syndesmosis on testing(Hunt et al, 2013)
Management
Once the grade of injury is identified, an individualised treatment plan is developed for all patients in our clinic to help them reach their goals of returning to ADL’s, sport and general activity.
Management is dependent on the severity of the ligament injury and grade of the tear.
Grade I-II syndesmosis injuries can be managed conservatively with physiotherapy, as long as there is no instability of the ankle. Initial management for Grade I-II injuries includes the use of an ankle brace or a CAM boot (moon boot) to provide stability and protection, while allowing the patient to put weight through their foot (Miller et al, 2014 & Hunt et al, 2013). The use of crutches can assist with promoting reduction in pain and allow you to safely move around.
With an unstable Grade II or Grade III injury, patients potentially require surgery to prevent further instability and injury to the joint. In this instance, we will contact your GP to organise a referral to an orthopaedic surgeon for opinion and management. Misdiagnosing an unstable syndesmosis injury will correlate with poorer outcomes and can lead to arthritis in the ankle later in life.

Rehabilitation
Rehabilitation can start on day 1 post-injury if a fracture is not suspected. Furthermore, it can be split into 3 phases:
Phase 1:
Rehabilitation can start on day 1 post-injury if a fracture is not suspected. The first phase in rehabilitation focuses on promoting healing to protect the joint and a CAM boot or bracing is typically provided. Phase 1 also aims to reduce inflammation and maintain ankle mobility through this protection phase while integrating safe (typically non-weight bearing) strengthening exercises.
Phase 2:
The second phase of rehabilitation concentrates on improving movement, regaining a normal walking pattern, restoring strength, and aiding a return to normal activities of daily living (domestic tasks, commuting to work, grocery shopping etc.). This stage is primarily focused on addressing any movement compensations that have occurred from walking with a limp or being immobilised in the CAM boot. Furthermore, this subacute phase of rehabilitation includes balance training with exercises performed on unstable surfaces such as wobble boards, air cushions and air-filled domes (Williams & Adams 2010). Balance training is important in the ankle helping to reduce the risk of re-injury in the future.
Phase 3:
The third phase of rehabilitation occurs when the patient can jog and hop on the injured ankle without pain or instability (Williams & Allen 2010). This phase incudes agility training, plyometric work, and running retraining. Our physiotherapists also evaluate a patient’s biomechanics and the kinetic chain to ensure successful return to sport and prevention of subsequent injuries. End stage rehabilitation involves guiding the patient back to a safe return to sports. This requires the player to perform sports specific drills and participate in full training including full contact at actual game speed with good quality movement and minimal discomfort (Williams & Adams 2010). Often a return to sport is achieved initially with the use of taping or bracing to prevent further injury.

Conclusion
An accurate diagnosis including grade of the injury is integral to successful management and prognosis of syndesmosis injuries. Poor rehabilitation in Grade I-II ankle injuries results in 30-70% of patients reporting persistent pain, ongoing time away from work and sport and can also result in impairments in activities of daily living. With no rehabilitation or poor management, these ongoing limitations can range from 6 months to seven years post injury (Brison et al, 2016). It is also important to note that rehabilitation of a syndesmosis injury can take up to twice as long as a normal lateral ankle sprain (Van Dijk CN et al. 2016).
In the instance that surgical management is required, a similar process of rehabilitation and recovery is achieved, but simply with a slightly different timeline as outlined by the specific surgeon’s protocol.
Research indicates that the period of immobilisation should be followed by a gradual and staged rehabilitation and return to sport program to reduce the risk of re-injury and development of premature ankle arthritis which occurs in 40% of unstable syndesmotic injuries (D’Hooghe P, et al 2020).
Ultimately Syndesmosis injuries can be treated with great success by our team at Five Dock Physiotherapy & Sports Injury Centre, but timely assessment, diagnosis and management is critical to achieve great results and positive patient outcomes.
HAVE YOU INJURED YOUR ANKLE?
GET AN ASSESSMENT & TREATMENT WITH OUR AMAZING PHYSIO TEAM.

- Get crystal clear on about what’s causing your pain or injury
- Understand what activities you can do without suffering consequences of ankle pain or ongoing ankle issues
- Find out the simple yet essential exercises that can help you achieve the best results
- Leave the session with the confidence of knowing exactly what to do to help you get symptom free and back to sport and activity living life without pain & dysfunction