Hip impingement, also known as femoro-acetabular impingement (FAI), is a condition that occurs when there is abnormal contact between the femoral head (the ball of the hip joint) and the acetabulum (the socket of the hip joint). This contact can cause damage to the joint, pinching and lead to pain and limited range of motion. FAI affects both men and women and is most common in young active individuals, particularly athletes (Fotier et al. 2022). Studies have shown that the prevalence of FAI is approximately 10-15% in the general population, and up to 30-40% in athletes (Zhang et al. 2015).
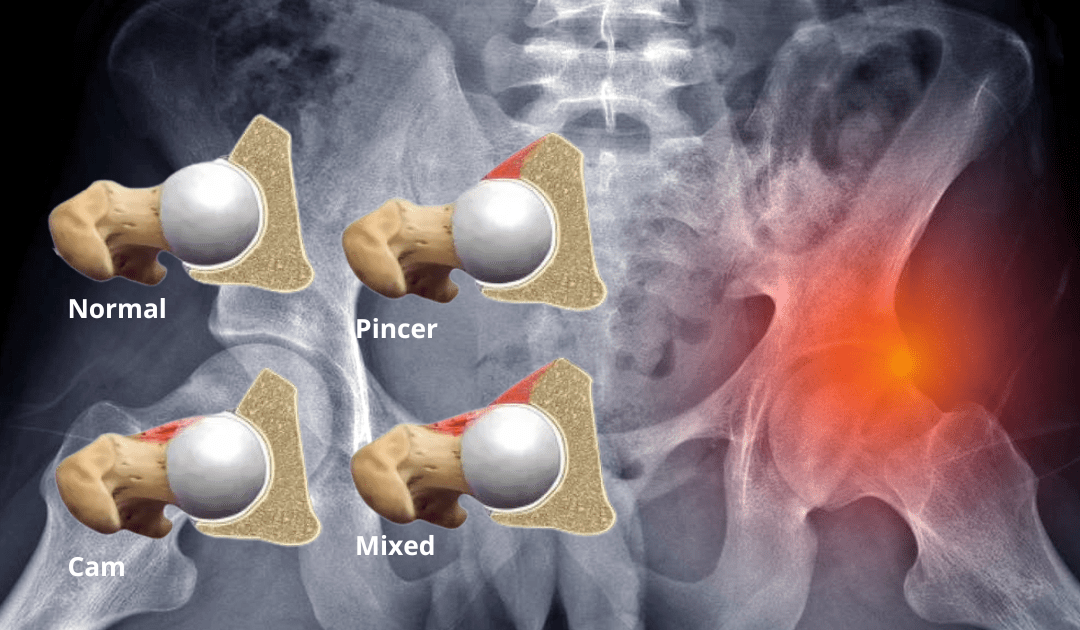
FAI can be divided into two main categories: Cam impingement and Pincer impingement. Cam impingement occurs when there is an abnormal shape of the femoral head, which can cause it to rub against the acetabulum during hip movements. Pincer impingement, on the other hand, occurs when there is an overgrowth of the acetabulum, causing it to cover more of the femoral head than usual. In some cases, both types of impingements may be present.
People with hip impingement may have been born with a structurally abnormal ball-and-socket joint or, the hip joint may have become structurally abnormal (or may be progressing towards becoming structurally abnormal) through repetitious activity. This typically involves recurrent movement of the legs beyond the normal range seen in certain athletes (football, baseball, soccer, tennis, hockey, lacrosse players, dancers, and golfers). An injury may also cause symptoms of hip impingement.
Diagnosis
FAI is typically diagnosed following a physical examination, often performed by a physiotherapist. The testing will include a gait assessment, hip active range of motion, FADIR (flexion, adduction & internal rotation of the hip) and Thomas test. This occurs alongside an assessment of muscle activation and lumbo-pelvic-hip stability, hip and lower limb strength, and biomechanics. An X-ray can help identify any abnormalities in the shape of the hip joint, such as cam or pincer morphology, which may be contributing to impingement.
Causes/Risk factors
- Hip anatomy: Certain variations in hip anatomy such as CAM or Pincer morphology can contribute to FAI.
- Age: FAI is most common in young adults between 20-40 years of age
- Hip muscle weakness/imbalance leads to reduced hip joint support and can lead to impingement.
- Poor hip and lower limb biomechanics/kinetic chain dysfunction
- Repetitive hip flexion movements in activities such as running or cycling.
- Prolonged periods of sitting
- Obesity can lead to more load on the hip joint.
Physiotherapy management
Physiotherapy is often used as a first-line treatment for FAI. Some of the most common physiotherapy modalities for FAI include manual therapy, exercise therapy, and hip joint mobilization. Recent evidence has shown that physiotherapy can be effective in reducing pain, improving hip function, and delaying or even preventing the need for surgery in some cases (Kemp et al., 2021). Additionally, specific exercise programs that target hip muscles can help reduce the risk of re-injury and improve overall hip function.
Studies have shown that manual therapy can be effective in reducing pain and improving hip function in individuals with FAI (King et al., 2015 & Kim et al., 2020). This includes both soft tissue massage of the surrounding muscles as well as hip joint mobilisations (Mehraram et al., 2020).
Specific exercises can be prescribed to target the hip muscles and improve hip stability, mobility, and strength. Studies have shown that exercise therapy can be effective in reducing pain, improving hip function, and delaying or preventing the need for surgery in individuals with FAI (Kuhns et al., 2019)
Addressing the kinetic chain is an important aspect of physiotherapy management for FAI as it allows for a comprehensive approach to identifying and addressing any underlying movement dysfunctions that may contribute to the development or exacerbation of FAI. In a recent study by Shapira et al. (2021), the authors demonstrated that addressing the entire kinetic chain, including the lumbar spine and lower extremities, was effective in reducing pain and improving hip function in individuals with FAI. Specifically, the authors found that a combination of hip-focused and lumbar-focused exercises, as well as lower extremity-focused exercises, resulted in significant improvements in pain and function in individuals with FAI.

Physiotherapy Exercises to help with FAI
Clams:
Aim: Gluteus Medius training incorporating core control. This strengthens up and stabilises the hip training these muscles.
How do I do the exercise? Lye on your side with your knees bent to 90⁰ stacking your shoulder, hips and feet in one line. Keeping your heels together and with your core engaged, lift the top knee, engaging your gluteus medius muscle. Hold for 5 seconds and repeat for reps.

Scissors with hands in straps:
Aim: Improve lumbo-pelvic-hip stability and hip dissociation, training the anterior oblique sling.
How do I do the exercise? Lye supine on the reformer with core engaged and feet starting in the tabletop position. With core remaining on, and knees maintaining a 90⁰ bend, move from the hip so as to alternately tap your toes. For more core activation and use of posterior oblique sling add hands in straps or a plough movement.

Kneeling Hip flexor stretch:
Aim: To stretch out the Rectus Femoris, iliacus and psoas muscles that often get tight in FAI patients.
How do I do the exercise? Start in a kneeling lunge position with both knees at 90 degrees. Engage your ‘Tucking your tail’ pushing the bottom forward. Stay tall as you slowly transfer your weight forward, stretching the back leg. Hold for 30 seconds.
